Reference: Miller TL, Curatolo C. Proximal tibiofibular joint instability: An underrecognized cause of lateral knee pain and mechanical symptoms. Journal of the American Academy of Orthopaedic Surgeons. Published online March 1, 2023. doi:10.5435/jaaos-d-22-01013
Abstracted by: David Ryland, PT, DPT, OCS, COMT, Anchorage, Alaska – Fellowship Candidate, IAOM-US Fellowship Program & Jean-Michel Brismée, PT, ScD, Fellowship Director, IAOM-US Fellowship program.
PART 1:
Context: The proximal tibiofibular joint is an underrecognized joint that can cause lateral knee pain and instability. The authors go in-depth about the etiologies, risk factors, patient presentation, diagnostic criteria, and treatment options that include both conservative and surgical.
Objective: The purpose of the study was to review the anatomy, pathoanatomy, and treatment strategies of the PTFJ.
Type of Review: Review article
Details of Paper: The purpose of the PTFJ is that it provides profound tensile stability to resist fractures of the of fibula when loads are applied to the lower extremity. There are two anatomical variations of the PTFJ: horizontal and oblique, with the oblique variation being more common to develop an instability. The PTFJ moves slightly in both anterolateral to posteromedial direction and internal / external rotation during both ankle and knee motions. The main risk factors to developing an instability include trauma, congenital ligamentous laxity, and sports aggressive rotational sports.
There are five different types of PTFJ instabilities:
- Anterolateral dislocation – Most common with a mechanism of injury of sudden inversion of a plantarflexed foot with knee flexion and external rotation of the leg.
- Posteromedial dislocation – Second most common and are associated with fibular nerve irritation.
- Superior and inferior dislocation – Very rare occurring from high energy trauma
- Subluxation – Excessive anterior to posterior motion without dislocation.
PTFJ instability can be diagnosed clinically with joint play (Figure 1) and the Radulescu sign, which is best performed with the patient prone, with one hand of the examiner stabilizing the thigh and the knee flexed to 90 degrees, while the other hand internally rotates the leg in an attempt to subluxate the fibula anteriorly (Figure 2).1,2 Diagnostic imaging can confirm with standard anterior-posterior and lateral radiographs.
Conservative treatment should be performed initially, which includes bracing / taping, anti-inflammatories and strengthening lower extremity musculature. Surgical options include arthrodesis, fibular head resection, open reduction with internal fixation, and ligament reconstruction with soft tissue grafting.


Figure 1: Joint play testing of the proximal tibiofibular joint Figure 2: Radulescu sign
Main Outcomes: Conservative treatment should be performed initially, which includes bracing / taping, anti-inflammatories and strengthening lower extremity musculature. Surgical consultation and stabilization should be performed after plateauing in conservative care. In cases of arthritis, an arthrodesis would be considered best practice. In cases of young athletes, a ligament reconstruction with soft tissue graft is considered best practice.
Application: This article is geared towards all clinicians who may see this pathology. It provides a review of the literature on an underdiagnosed pathology and provides information that can be utilized immediately. The flow chart provides an excellent visual for the recommended treatment algorithm for those with acute versus chronic PTFJ instability.
Conclusions: PTFJ instability can cause lateral knee pain, a sense of instability, and mechanical symptoms that is often overlooked and misdiagnosed in the clinical setting. There are multiple types of instability with the most common being anterolateral dislocation. There is a paucity of literature for the successfulness of treatment methods for the PTFJ instability, especially conservative treatment methods.
PART 2:
Clinical Relevance: The information gleaned from this study is pertinent to clinicians. The PTFJ instability is a highly underdiagnosed pathology that can cause lateral knee / vague anterior shin pain. It is often misdiagnosed as meniscal pathology, lateral collateral ligament pathology, chondral injuries, posterolateral rotatory instability, and biceps femoris tendopathy, and thus, not successfully managed. This study brings awareness to the pathology and provides treatment options for both conservative and surgical healthcare providers. Using a modified version of the PTFJ taping method that is taught in the International Academy of Orthopedic Medicine – US (IAOM-US), may serve as a conservative intervention to facilitate return to a prior level of function (Figure 3).
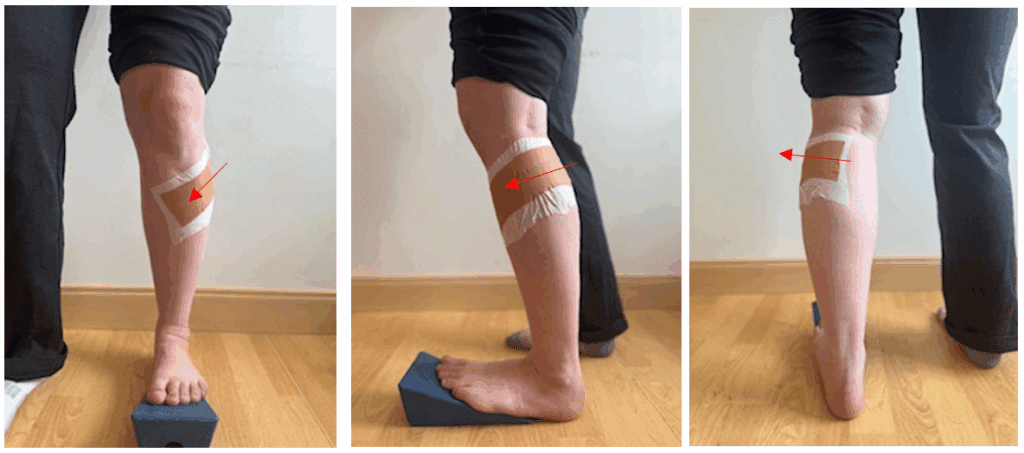
Figure 3: Modified technique of the IAOM-US taping of the proximal tibiofibular joint
Content Consistency: There is a gap in the literature regarding this pathology. This review article took the most relevant information about the PTFJ regarding anatomy, pathoanatomy, diagnosis, and treatment.
References
- Phelps V. Differential Diagnosis and Musculoskeletal Management of the Knee – Lateral Pain. lecture presented at: International Academy of Orthopedic Medicine – US Knee Course.
- Abreu FG, Andrade R, Pereira R, Bastos R, Espregueira-Mendes J. Evaluation of the Stability and Function of the Tibiofemoral and Tibiofibular Joints. In The Art of the Musculoskeletal Physical Exam 2023 Jun 17 (pp. 443-457)